The approach to treating an enlarged prostate is changing. For years, options for Benign Prostatic Hyperplasia (BPH) were often limited. Patients could manage symptoms with medication or consider traditional surgery. Many men felt stuck between frustrating daily symptoms and a highly invasive procedure. That landscape looks very different today.
The focus has shifted to minimally invasive treatments that preserve quality of life. This is where the conversation around prostate artery embolization in Colorado has evolved. It’s no longer seen as just an alternative procedure. For many, it has become a primary, effective option for relieving BPH symptoms without the risks of major surgery. It addresses the root cause by reducing blood flow to the prostate.
But with more options comes more confusion. Patients need to know how to evaluate this treatment. This guide provides clear, direct information about what makes someone a good candidate and what specific questions to ask a specialist.
Quick answer: Prostate artery embolization (PAE) is a minimally invasive, outpatient procedure. An interventional radiologist uses image guidance to block the arteries that supply blood to the prostate. This causes the gland to shrink, relieving urinary symptoms caused by BPH.
What’s inside
- How Does Prostate Artery Embolization in Colorado Actually Work?
- Are You a Good Candidate for This Procedure?
- Comparing PAE to Traditional Surgery (TURP)
- What Key Questions Should You Ask Your Interventional Radiologist?
How Does Prostate Artery Embolization in Colorado Actually Work?
The treatment is administered through a tiny puncture in the wrist or groin, not a large surgical incision.
An interventional radiologist performs the entire procedure through that pinhole opening. The specialist starts by numbing a small area, usually on the wrist. Then, a very thin, flexible tube called a catheter is inserted into the artery. The patient remains awake but comfortable, often with light sedation.
This is where the “image-guided” part is crucial. The specialist uses advanced X-ray imaging, called fluoroscopy, to see the patient’s arteries in real time. It acts like a live GPS map inside the body. The catheter is carefully navigated to the specific arteries supplying blood to the prostate.
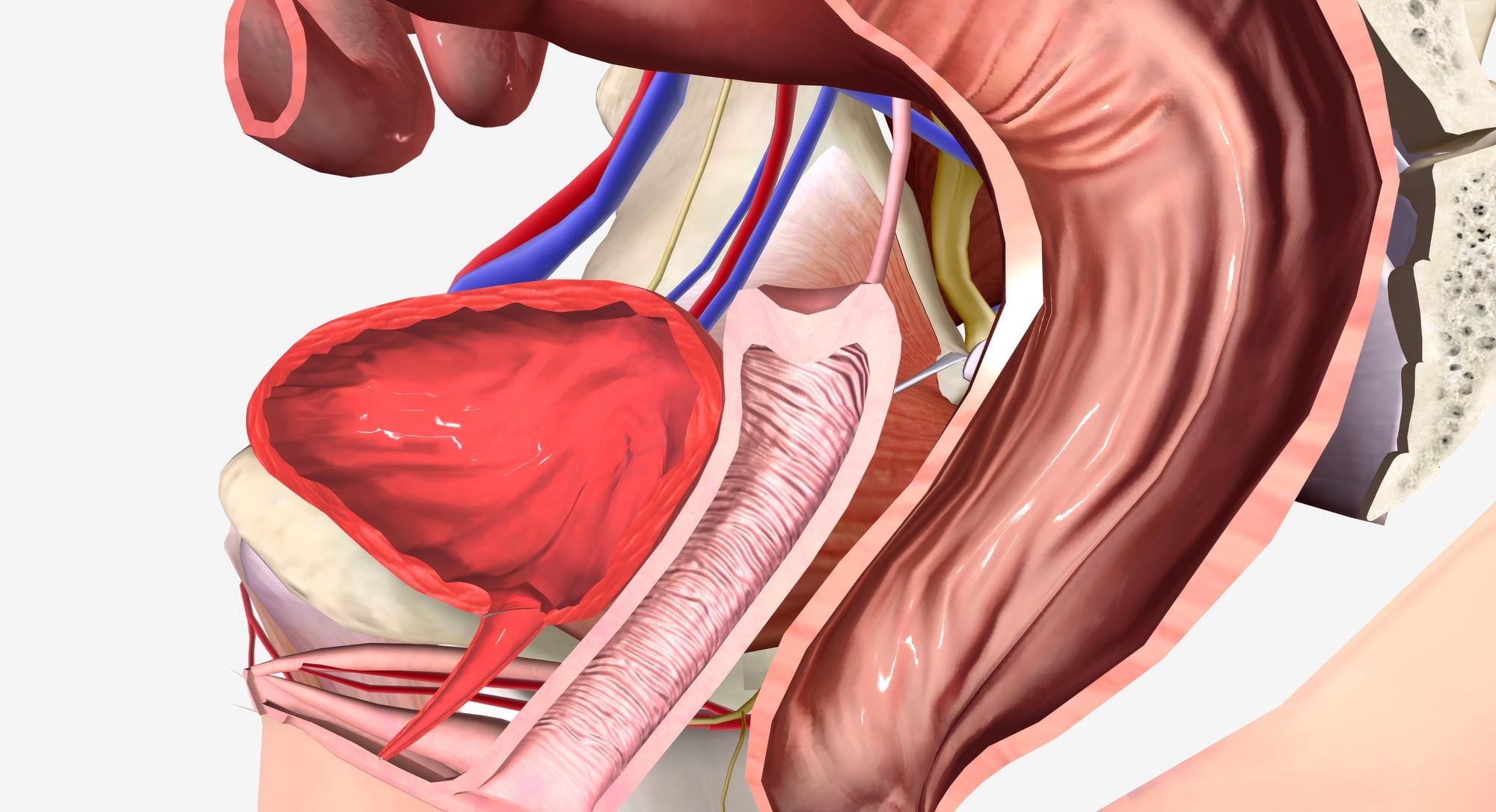
Once the catheter is perfectly positioned, the doctor releases microscopic, sand-like beads. This process is called embolization. These beads flow into the small vessels and block blood supply to the enlarged parts of the prostate. Deprived of oxygen and nutrients, the prostate tissue begins to shrink over the following weeks, with clinical studies per PMC showing a 20-40% reduction in prostate volume. Visualizing the process can help. Diagrams and further details on prostate artery embolization Colorado show how it’s done.
❝ The key to a successful PAE isn’t just blocking an artery. It’s precisely mapping the patient’s unique arterial anatomy. This ensures only the prostate tissue is targeted, protecting the bladder and rectum.
After blocking the arteries on both sides, the catheter is removed. A small bandage is placed over the entry point. The entire outpatient procedure typically takes a few hours. Patients can go home the same day to recover in comfort.
Are You a Good Candidate for This Procedure?
You are likely a good candidate if you have moderate to severe BPH symptoms and want to avoid major surgery.
The best candidates for PAE are typically men over 50 who are experiencing frustrating urinary issues. These include a frequent urge to go, a weak stream, or waking up multiple times at night. Often, these candidates have tried medications without getting the needed relief, or the side effects from those drugs are impacting their quality of life.
Overall health is also a factor. PAE is an excellent option for patients with other medical conditions that might make traditional surgery with general anesthesia too risky. Because it’s minimally invasive, it’s safer for men with heart or lung conditions. It’s also a strong choice for those on blood thinners that can’t be stopped for surgery.
❝ It is important to ask a specialist about prostate size. PAE is particularly effective for men with very large prostates (over 80 grams). Traditional surgery can be more difficult and riskier on larger glands. PAE, however, works by shrinking the entire gland, making size less of an obstacle.
Finally, a key factor is the desire to preserve sexual function. One of the biggest concerns with surgical options like TURP is the high risk of side effects, including retrograde ejaculation or erectile dysfunction. PAE has a significantly lower risk of impacting sexual health, making it a preferred choice if that is a priority. A Mint STL study of 630 patients treated with PAE found success rates of 81.9% at 1-3 years with no reports of sexual dysfunction or urinary incontinence.
Comparing PAE to Traditional Surgery (TURP)
Finding the right path involves comparing invasiveness, recovery, and potential side effects.
The choice for treating BPH isn’t just about symptom relief; it’s about how the treatment fits into your life. You will need to weigh the effectiveness against the recovery time and risks. Understanding the key differences between PAE and the surgical standard, TURP, is essential.
The Surgical Standard: TURP
Transurethral Resection of the Prostate (TURP) has long been the go-to surgery. A surgeon works through the urethra to physically cut away excess prostate tissue. It is very effective at opening the urinary channel. However, this approach requires a hospital stay and general anesthesia. The recovery period is longer and often more uncomfortable. Patients typically need a urinary catheter for several days after the procedure.
✓ Key Considerations:
- Requires a hospital stay of one to two days.
- Carries a higher risk of sexual side effects, like retrograde ejaculation.
- Full recovery can take four to six weeks.
The Minimally Invasive Option: PAE
Prostate Artery Embolization takes a completely different approach. It’s an outpatient procedure performed with light sedation, not general anesthesia. It doesn’t remove tissue. Instead, it shrinks the prostate by reducing its blood supply. This means a much faster recovery and a very low risk of complications. You can go home the same day and are often back to normal activities within a week.
✓ Key Considerations:
- Outpatient procedure with no hospital stay required.
- Very low risk of impacting sexual function.
- Quick return to daily life, often within a few days.
What Key Questions Should You Ask Your Interventional Radiologist?
You should come prepared with specific questions about a specialist’s experience, the procedure’s details, and long-term outcomes.
A successful outcome depends heavily on the specialist’s skill. The consultation is your opportunity to gain confidence in your chosen provider. It helps you understand the process and set realistic expectations. A good doctor will welcome questions and provide clear answers.
Questions About the Specialist’s Experience
This is the most important part of your research. The technology is only as good as the person using it. Look for a specialist who performs PAE regularly and has a deep understanding of pelvic arterial anatomy.
Here are the critical questions to ask:
- How many PAE procedures have you performed?
- What percentage of your practice is dedicated to PAE?
- Are you a board-certified interventional radiologist?
- Can you walk me through a typical case, from start to finish?
❝ You should ask to see anonymized before-and-after imaging from previous patients. A confident specialist can show how the prostate shrinks and how blood flow is reduced. This is tangible proof of their skill.
Questions About the Procedure Itself
Understanding the technical details can build your confidence and clarify what to expect on the day of the treatment. You should not be shy about asking for simple explanations of complex terms.
Ensure you get clear answers on these points:
- What type of imaging guidance do you use? The standard is fluoroscopy, which is a type of live X-ray.
- What kind of embolic particles do you use? These are the microscopic beads that block the arteries.
- Will you access the artery through my wrist (radial access) or groin (femoral access)? Why?
- What kind of sedation will I receive?
Questions About Outcomes and Recovery
Your goal is symptom relief and a better quality of life. You need a realistic picture of what happens after the procedure, including both the recovery period and long-term effectiveness.
Discuss these topics with your doctor:
- What is your personal success rate for symptom improvement?
- What are the most common side effects you see?
- How long will it take for me to notice a difference?
- What are the long-term results? A longitudinal study of 1,550 patients published by Mint STL found clinical success for symptom relief was 88.1% at 1 year and 76.8% at 6-10 years.
You should also ask about the chance of needing another procedure down the road. A 2024 Sci-Direct abstract reported a 10-year re-intervention rate of 20% for PAE alone. Knowing these numbers helps you set clear expectations for the future. This conversation is your best tool for making an informed decision.
Frequently Asked Questions About Prostate Artery Embolization
Here are direct answers to common questions about the procedure, insurance, and what to expect.
Decision FAQs
Does insurance typically cover prostate artery embolization? Yes, most insurance plans, including Medicare, now cover PAE. It is a recognized treatment for BPH. The specialist’s office will handle the pre-authorization process, which confirms coverage before the procedure is scheduled.
What is the risk of serious complications from prostate artery embolization?
Minor side effects like temporary urinary symptoms and fatigue are common after PAE. Serious complications are rare but can include non-target embolization. An experienced interventional radiologist minimizes these risks through precise catheter guidance.
❝ This article is for general educational purposes only and is not medical advice. Outcomes vary by individual. Consult a qualified healthcare professional before making decisions about your care.