Fibroids are non-cancerous smooth muscle tumors that grow in the muscle of the uterus. They are more common than most people think and can cause problems with your menstrual cycle including pain, bleeding, frequency of urination, pelvic pressure and back pain. Fibroids can also cause infertility by preventing growth of the embryo – or pregnancy – into the uterine lining and by blocking the fallopian tubes.
Many women with pain and bleeding actually may have fibroids, which can be easily diagnosed by an ultrasound. Ultrasound is convenient, inexpensive, much more accurate than a pelvic exam, and relatively easy to tolerate. When pain or bleeding occurs with the period, an ultrasound should always be performed since it is one of the most accurate ways to detect fibroids located anywhere in the uterus.
OBGYN’s are often the first doctors that identify fibroids in patients, and in many cases a “watch and wait” approach is used. The OB may tell the patient that the fibroids are small and are not causing many problems at present, or they will be treated once they are interested in pregnancy.
The problem – fibroids grow because estrogen in the ovaries makes them grow. This means that fibroids will continue to grow as long as your ovaries are making estrogen, and they will cause more symptoms the larger they become. Heavier bleeding will cause anemia, pressure from the fibroids can affect your bladder and bowel causing you to “pee” more frequency as well as diarrhea or constipation. Bloating and distension, pelvic pressure and back pain become worse as well. Your menstrual cycle will often become more and more painful.
Your OBGYN may prescribe birth control pills to try and control bleeding. Realize that this is only a temporary solution, since birth control pills have estrogen and the fibroids will continue to grow.
So what should you do?
Treatment of Fibroids – What is the BEST Option?
Fibroid treatment depends on many factors. The most important is whether or not the patient wants to become pregnant. For those who are past childbearing or do not want pregnancy, there are more options available. However, if pregnancy is desired, the options are very limited. The following discussion will focus on those patients who desire fertility and preservation of the uterus.
Fibroid Removal Surgery – The Best Option
Removal of fibroids from the uterus, also called “myomectomy,” is the best option for immediate relief of symptoms and for preservation of fertility. Fibroid removal surgery will preserve uterine structure and function, and immediately stops heavy bleeding, pain, frequency of urination, pelvic pressure and back pain.
Uterus Before Myomectomy
In this diagram, the fibroids are large and are pushing against the bladder, which is being pressed against the pubic bone. The result is a decrease bladder capacity causing frequency of urination. The fibroids also press against the back causing back pain, extend to the abdomen causing distension and bloating, and can also push against the colon causing constipation and diarrhea. Fibroids impact the uterus by irritating the uterine lining and increasing the size of the uterus and the lining resulting in heavy bleeding and pain with cycles. Fertility can be affected since the fibroids will prevent implantation of the embryo to form a pregnancy as they get larger, so removal often helps to increase pregnancy rates.
Uterus After Myomectomy
Fibroid removal brings the uterus back to normal size and shape and eliminates all the symptoms present before the surgery as noted above. It is important that any fibroid removal surgeon ensures the patient that ALL fibroids will be removed, other than very small “seedling” fibroids. Leaving moderate or large fibroids in the uterus does not help symptoms are fertility chances. Always ask your OBGYN or Surgeon how they are removing fibroids from your uterus, and whether or not they are removing all of the fibroids during the procedure.
Less Effective Options
Embolization is a fibroid treatment option that has potential negative effects on the uterus. With embolization, plastic particles are injected into the blood supply of the fibroids in an attempt to “kill” the fibroids. Since embolization does not remove fibroids, they remain in the uterus and can increase the risk of miscarriage, or pregnancy loss. Embolization also has the potential to decrease blood flow to the ovaries resulting in earlier menopause.
Fibroids Before Embolization
Fibroids After Embolization
Embolization does NOT remove fibroids, but blocks their blood supply in an attempt to “kill” fibroids. Dead fibroids cause significant pain, with most patients indicating that embolization often causes much more pain than the LAAM surgery for fibroid removal, and it lasts longer. Embolization will NOT result in immediate relief of symptoms, and may take months or years to resolve symptoms. Further, embolization can affect rates of miscarriage by increasing them since the fibroids are not removed, and can also potentially impact blood flow to the ovaries and affect fertility.
Radiofrequency ablation is a technique where a probe is placed into the fibroid and the fibroid is heated up in an attempt to kill the fibroid. This technique also should not be used for fertility since it can damage the uterus.
MRI guided ultrasound is another technique that relies on destruction of the fibroid while the fibroid is in the uterus.
For any procedure that is used to treat fibroids, it is always best to remove the fibroid rather than use a procedure that keeps the fibroid in place if fertility is desired.
The Best Fertility Option
There are certain types of fibroid removal procedures that can result in recovery times and results with less pain that are actually BETTER than embolization, radiofrequency ablation (Accessa, Sonata) and other types of procedures that attempt to kill a fibroid rather than remove it. LAAM – Laparoscopic Assisted Myomectomy – is an example of a fibroid removal procedure that removes ALL fibroids from the uterus of ANY size, immediately relieves symptoms, uses a very small incision with a recovery of 7 to 10 days, and allows for less pain and better outcomes.
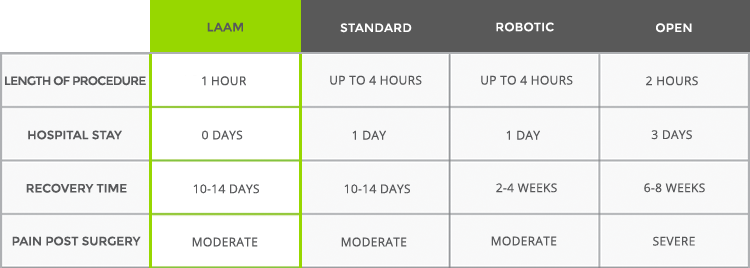
LAAM-BUAO COMPARED WITH OTHER PROCEDURES BASED ON SIZE OF THE FIBROIDS
LAAM-BUAO COMPARED WITH OTHER PROCEDURES BASED ON THE NUMBER OF FIBROIDS
OVERALL BENEFITS OF LAAM-BUAO COMPARED TO OTHER PROCEDURES
Always consider fibroid removal procedures when fertility is a consideration. It is your best option for the fastest recovery, immediate relief of symptoms, the least amount of pain, and will preserve the uterus and ovaries.
The LAAM Procedure – Laparoscopic Assisted Myomectomy – and Why it is the BEST Option for Fibroid Removal
There are many ways to perform fibroid removal from the uterus.
Open Myomectomy (Laparotomy – Large Incision)
The standard way is to make an open incision, remove the uterus from the pelvis so that it is “sitting” on the tummy, and then remove the fibroids. With the fibroids removed the uterus is much smaller, and is replaced back through the large incision. With this approach, a large incision is required to remove the large uterus, since the fibroids are making the uterus much bigger than normal. For example, a uterus with three large fibroids each at 7 cm is roughly THREE TIMES LARGER than a normal uterus, and a large incision is required to remove it to perform open myomectomy. Open myomectomy requires a recovery time of three days in the hospital, and then 8 weeks before most patients are at 80% normal.
Laparoscopic Myomectomy (Minimally Invasive – two to five+ smaller incisions)
There are three main ways to perform laparoscopic myomectomy – standard, robotic, and LAAM.
Robotics
Robotic myomectomy is not a great option. With all the technology used to develop robotics and the higher cost to the patient and the healthcare system, robotics just are not well matched for fibroid removal.
The LAAM Procedure
LAAM is a “hybrid” approach to fibroid removal, using the best results with open surgery matched with incisions that are smaller in number in size than either robotic or other laparoscopic approaches. LAAM provides a “revolutionary” way to remove fibroids that is safe, very effective, and has the fastest recovery of ANY fibroid removal procedure. These results have been published in a comparison trial between open, robotic, and laparoscopic approaches, with the references here.
Why isn’t LAAM Used MORE?
LAAM is a highly specialized procedure that requires a significant amount of training and expertise to perform properly. Once mastered, LAAM becomes a superior option for patients requiring fibroid removal for both symptomatic relief and for fertility. Other options simply do not compare.
The surgeons at the Center for Innovative GYN Care developed and perfected LAAM procedures with the application of a laparoscopic tourniquet, and with time and experience have been able to improve and refine the procedure to provide almost all patients with the LAAM option to greatly improve their condition and outcome. There really is no substitute for training and experience in surgery. LAAM is an example of a procedure that when performed properly results in amazing outcomes. When performed improperly by those who have do not have the experience and training, the results are not optimal.
Realize that OBGYN’s do not perform enough surgery to master the technique and training that LAAM requires. The same is true for many “Specialists.” Consider a consult to the surgeons of CIGC for more information and a discussion of the LAAM option for treatment of your condition.